Patella Dislocations & Medial Patellofemoral Ligament Reconstruction (MPFL)
A board-certified, fellowship-trained orthopaedic knee surgeon and sports medicine specialist, Dr. Steven Chudik is renowned for his arthroscopic knee expertise and innovative procedures that reduce surgical trauma, speed recovery and yield excellent outcomes.
Through his research, Dr. Chudik investigates and pioneers advanced and novel arthroscopic procedures, instruments and implants that have forever changed patients’ lives. Never content to settle for what’s always been done for orthopaedic knee care, Dr. Chudik prides himself on providing individualized care and developing a plan that is right for each patient. By taking this approach for the past 20 years, Dr. Chudik has developed minimally invasive surgical techniques and instruments, as well as injury-specific rehabilitation programs and return to sport and activity protocols and testing.
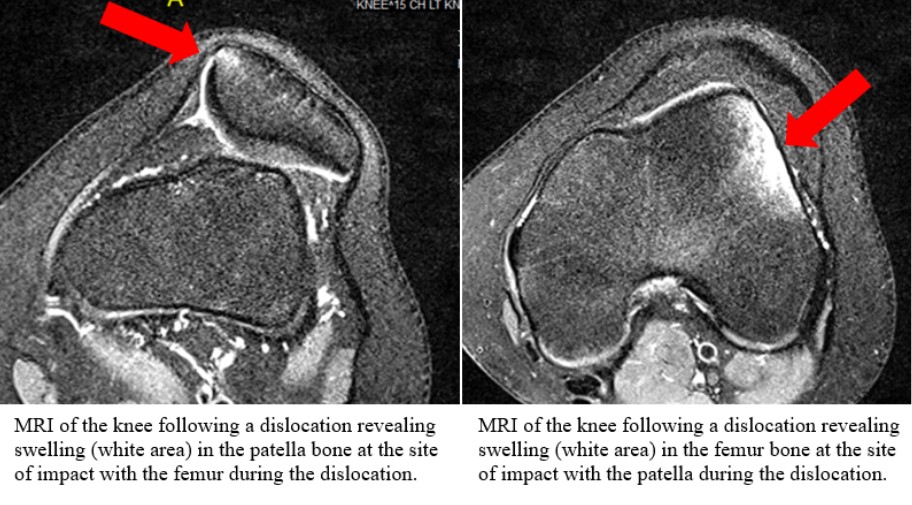
When the patella (knee cap) is dislocated, the structures on the medial side of the patella are torn. Often after a dislocation, the knee can be rehabilitated in physical therapy and the patient can attempt to return to activities. However, some patients continue to experience instability and dislocations. With each dislocation, there is a risk for associated injuries to the cartilage in the knee. After proper conservative treatment, if the patient continues to have recurrent dislocations, surgery to reconstruct the MPFL is recommended.
Patellar Tendon Expertise
Non-operative treatment of Patella Dislocations
MPFL Reconstruction
Cartilage Repair
Quadriceps Tendon Injuries
Patellar Tendon Injuries
Return to Sport Testing
Return to Sport Training Program

Individualized Treatment and Rehabilitation
Because no two people and no two injuries are alike, Dr. Chudik uses his expertise to develop and provide individualized care and recovery plans for patients. This customized attention explains why patients travel to have Dr. Chudik care for their knee conditions and injuries. Dr. Chudik developed treatments, rehabilitation and even return to activity protocols for football, soccer, volleyball, lacrosse, golf, baseball, tennis, and other activities and sports. He also developed and is a knee functional test to provide a definitive test to determine when it is safe for patients to return to sport following a knee injury.
Frequently Asked Questions
A patellar dislocation occurs when the kneecap (patella) moves out of its normal position in the knee joint, usually shifting laterally toward the outer side of the leg. This can cause intense pain, swelling, and a visible deformity to the knee. The patella normally sits in the trochlea (groove) on the femur (thigh bone) and is held in place by various soft tissues, including ligaments. When the patella dislocates, it damages the restraining ligaments and tissues.

Patellar dislocations occur during sports or activities that involve sudden changes in direction or with a direct blow to the knee. Structural issues, such as a shallow trochlear groove, and weak quadriceps muscles, limb malalignment, or an abnormally positioned patella can contribute to dislocations. People with these predisposing structural issues can experience dislocations with less trauma or even during routine activities.
The signs and symptoms of a patellar dislocation include:
- Intense pain in the knee
- Visible deformity when the kneecap is out of place
- Swelling and bruising around the knee
- Difficulty moving the knee or bearing weight
- A feeling of the knee “giving out” or instability
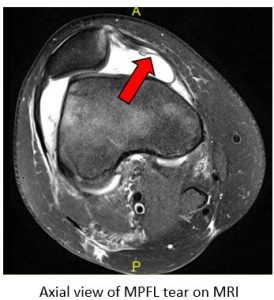
Diagnosis is based on a combination of the patient’s history, physical examination, and imaging studies. A healthcare provider will ask about the injury mechanism and symptoms, perform a physical exam to assess the stability of the patella, and order imaging tests like X-rays and MRI. These tests help confirm the dislocation, check for fractures, other injuries, and assess damage to the surrounding soft tissues.
Surgery may be necessary if:
- The dislocation is recurrent, meaning it happens multiple times.
- There is significant damage to the ligaments, cartilage, or bone.
- Non-surgical treatments like physical therapy or bracing fail to stabilize the knee.
Dr. Chudik will recommend the best treatment option based on the specific circumstances, including the severity of the dislocation, your activity level, and the condition of the surrounding knee structures.
Several surgical options are available, depending on the underlying cause of the dislocation.
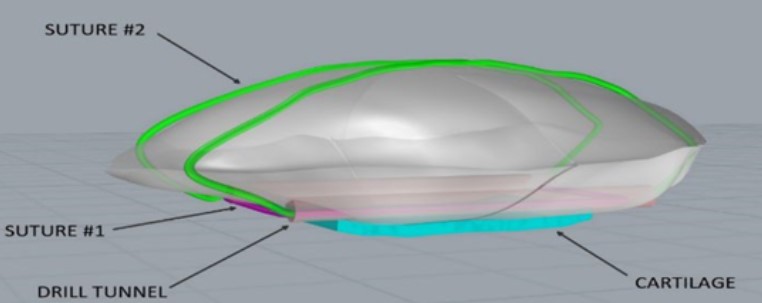
Medial Patellofemoral Ligament (MPFL) Reconstruction is the most popular and successful procedure which involves reconstructing the MPFL, a key ligament that helps keep the patella in place. A soft tissue tendon graft, often the hamstring, is used to replace the damaged ligament.
The surgery is usually performed as an outpatient procedure (go home the same day) with limited general anesthesia and an adductor canal nerve block. With MPFL reconstruction, a patient can expect to be on crutches initially and may bear weight on the surgical extremity as tolerated. There is no brace used to avoid atrophy (weakening) of the muscles. The incisions should be kept clean and dry for the first 10 to 14 days after surgery. Showering lightly is allowed after 2 weeks but the wounds cannot be submerged under water for at least 3 weeks after surgery. Physical therapy will be required to restore motion, strength, and proprioception (balance) following surgery and return to sports may take anywhere from 4 to 6 months.
A patient may return to light (sedentary) work or school within a week after surgery if the pain is tolerable and you are able to elevate your leg appropriately. It is important to avoid “overdoing it” with the involved leg during this time to avoid aggravation. Additionally, it is imperative that the patient work on restoring full knee extension and quadriceps muscle function with frequent stretching and exercises.
After the knee is fully rehabilitated, Dr. Chudik’s Return to Sport Testing protocol is performed to determine that the knee is fully rehabilitated and more importantly, that any errors in movement patterns known to put patients at risk for knee injury are corrected. Once this assessment is successfully completed, they may return to sport activity. Timelines for return to sport vary depending on the patient’s sport and position. Athletes often require 6 months for full clearance to sport participation.
With proper rehabilitation and ongoing strength training, patients experience significant, improvement in knee stability and function and a full return to activity is expected. However, there is an increased risk of future arthritis, particularly if cartilage damage occurred during the dislocation. There are no restrictions on activity.
Testimonials and Patient Stories

Active mom returns to pain-free life following overdue shoulder surgery.

Fate and a torn rotator cuff are changing the lives of countless orthopaedic patients

Daily commute gives active businessman, avid golfer an unexpected ride

Second shoulder work injury jeopardized Kucera’s job, bow hunting pastime
Knee Anatomy
Your knees are the most commonly injured joints in your body. Unlike your shoulder that moves in all directions, your knees appear only to bend and straighten, but actually their movements are much more complex and involve rotation, translation, sliding and rolling.
Ligaments
There are four main ligaments connecting the bones at the knee joint and provide stability when you walk, run and jump. They are the:
Anterior cruciate ligament (ACL)
Posterior cruciate ligament (PCL)
Medial collateral ligament (MCL)
Posterolateral corner (PLC) ligaments including the lateral collateral ligament (LCL)
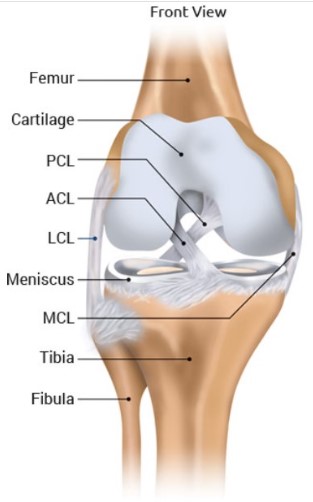
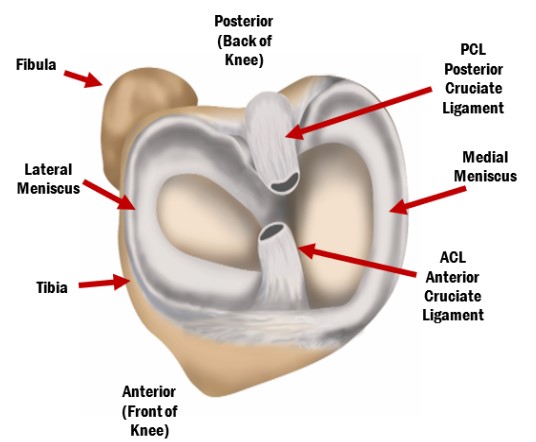
Cartilage and Meniscus
The joint surface of the knee is covered with a thin, but durable layer of cartilage over the ends of the femur, tibia and patella and, along with the meniscus, allow the knee surfaces to articulate, move smoothly—almost frictionless and painlessly along each other. The cartilage lacks a blood supply and recieves nutrition from the joint fluid. The meniscus has an unlimited blood supply. Without a blood supply and because of their relatively less active cellular makeup, the cartilage and meniscus do not maintain themselves. The cartilage and meniscus are extremely durable, but in time with “wear and tear” or following injury, they break down, fail, and lead to meniscus tears, cartilage damage and eventually symptomatic (pain, stiffness, swelling) arthritis (failure of this protective joint surface).
Tendons and Muscles
Tendons also help provide knee joint stability and movement. They act like strong cables connecting your muscles to your bones. These muscle-tendon units cross joints to compress, hold and move joints in specific directions. Like other parts of your knee, they are susceptible to injury and overuse. The two knee tendons most commonly injured are the quadriceps and patellar tendons.
Medial Patellafemoral Ligament
The medial patellafemoral ligament (MPFL) is most often injured by athletes when they dislocate their patella (kneecap) during activities that require pivoting, changing direction (cutting), jumping, or landing. The ligament runs from the patella (kneecap) to the femur (thigh bone) and is torn when the patella is dislocated.

Injuries & Conditions
Surgical Procedures
- Anatomic medial patellofemoral ligament reconstruction (MPFL)
- Patellar Tendon Repair and reconstruction after MPFL
- Quadriceps Tendon Repair and Reconstruction
- Patellar Tendonosis Debridement and Repair
- Bipartite Patella Repair/Excision
- Arthroscopic Assisted Patella Fracture Repair
- Non-Hardware, All-Suture Patella Fracture Repair
- Multiple Knee Ligament Repair/Reconstruction
- Tunnelless Onlay Patellar (kneecap) stabilization (Developed by Dr. Chudik)

About Dr. Chudik

- Curriculum Vitae (CV)
- Video
- Website: stevenchudikmd.com
- Schedule an appointment online
- Email: contactus@chudikmd.com
- Phone: 630-324-0402



Meet Dr. Steven Chudik
The Patient Experience
Innovation
Innovations
Through his research, Dr. Chudik investigates and pioneers advanced and novel arthroscopic procedures, instruments and implants that change patients’ lives because of better long-term outcomes, or outcomes that were never possible previously. His efforts continue to yield scores of patents that will positively affect orthopaedic surgical techniques worldwide.
Novel Procedures
- Tunnelless Onlay Medial Patellofemoral Ligament Reconstruction and Patellar (kneecap) stabilization (Developed by Dr. Chudik)
US Patents and Patent Applications
- Method of Minimally Invasive Shoulder Replacement Surgery, U.S. Patent No. 9,445,910, filed September 11, 2006
- Humeral Implant for Minimally Invasive Shoulder Replacement Surgery. Patent application serial number 11/529,185 case II, filed September 25, 2006
- Glenoid Implant for Minimally Invasive Shoulder Replacement Surgery, U.S. Patent No. 9,974,658, filed September 25, 2006
- Humeral Implant for Minimally Invasive Shoulder Replacement Surgery, Serial No.11/525,629, filed September 25, 2006, application published as U.S. Patent App. Pub. 2007/0016305 (A)
- Guide for Shoulder Surgery, U.S. Patent No. 9,968,459, filed September 29, 2006
- Suture Pin Device. Patent application serial number 11/529,2006, case XV, filed September 29, 2006
- Suture Pin Device, Serial No. 11/529,185, filed September 29, 2006, application published as U.S. Patent App. Pub. 2007/0027477 (A)
- Method of Arthroscopic or Open Rotator Cuff Repair Using An Insertional Guide For Delivering a Suture Pin, U.S. Patent No. 8,540,737, filed October 24, 2006
- Acromioclavicular Joint Repair System, U.S. Patent No. 9,387,011, filed February 2, 2007
- Resurfacing Implant for a Humeral Head, Serial No. 13/068,309, filed May 9, 2011, application published as U.S. Patent App. Pub. 2012/0041563 (A)
- Universal Anterior Cruciate Ligament Repair and Reconstruction System(Cannulated Scalpel), U.S. Patent No. 10,034,674, issued September 30, 2021
- Resurfacing Implant for a Humeral Head. Patent application serial number 13/068,309 case II (A), filed May 9, 2011
- Method of Arthroscopic or Open Rotator Cuff Repair Using an Insertional Guide for Delivering a Suture Pin. U.S. Patent Number 8,540,737 B2, issued September 24, 2013
- Cortical Loop Fixation System for Ligament and Tendon Reconstruction, Serial No. 13/998,567, filed November 12, 2013, application published as U.S. Patent App. Pub. 2015/0134060 (A)
- Acromioclavicular Joint Repair System. U.S. Patent Number 9,387,011 B2, issued July 12, 2016
- Method of Minimally Invasive Shoulder Replacement Surgery. U.S. Patent Number 9,445,910 B2, issued September 20, 2016
- Guide for Shoulder Surgery. U.S. Patent Number 9,968,459 B2, issued May 15, 2018
- Glenoid Implant for Minimally Invasive Shoulder Replacement Surgery. U.S. Patent Number 9,974,658 B2, issued May 22, 2018
- Glenoid Implant with Replaceable Articulating Portion, U.S. Patent No. 11,406,505, filed August 20, 2019, issued August 9, 2022
- Cortical Loop Fixation Method for Ligament and Bone Reconstruction, Serial No. 15/731,719, filed July 24, 2017, application published as U.S. Patent App. Pub. 2019/0021845
- Humeral Implant and Method, Serial No. 17/532,714, filed November 22, 2021, published as U.S. Patent App. Pub. US 2023/0157832
- Humeral Implant with Cannulation and Method, Serial No. 18/211,396, filed June 19, 2023
- Glenoid implant with Portal and Method, filed July 2023
Dr. Steven Chudik continually innovates to create new technology, and surgical techniques and improve patient care. He also collaborates worldwide with other leaders in the orthopaedic technology industry. Surgeries provide Dr. Chudik with an endless source of ideas to create new, safer, less invasive, and more effective surgical procedures, surgical instruments, and implants. Several of his shoulder patents are the direct result of these pioneering endeavors.
Research
An inquisitive nature was the impetus for Dr. Steven Chudik’s career as a fellowship-trained and board-certified orthopaedic surgeon, sports medicine physician and arthroscopic pioneer for knee injuries. It also led him to design and patent special arthroscopic surgical procedures and instruments and create the Orthopaedic Surgery and Sports Medicine Teaching and Research Foundation (OTRF). Through OTRF, Dr. Chudik conducts unbiased orthopaedic research and provides up-to-date medical information to help prevent sports injuries. He also shares his expertise and passion mentoring medical students in an honors research program and serve as a consultant and advisor for other orthopaedic physicians and industry.
Areas of Knee Research And Development